The Liabilities of Buprenorphine Treatment You Should Know About

In thousands of drug rehabilitation facilities across America, addiction treatment incorporates the use of buprenorphine, an opioid painkiller. While this drug is chemically similar to drugs like morphine, heroin and oxycodone, it is formulated to create less euphoria while still maintaining other opioid characteristics. Families seeking recovery for an opioid-addicted loved one are very likely to hear that treatment using this drug, referred to as medication-assisted treatment (MAT), is their best, if not only option.
This is certainly not the case and it’s important to know the whole story in order to understand the liabilities of this recommendation. In addition, there may be some usefulness to short term use of buprenorphine to ease withdrawal symptoms in individuals whose underlying health condition would make a withdrawal in any other way dangerous.
Buprenorphine Is Not Problem-Free
Buprenorphine in the various forms used in addiction recovery is an opioid similar to the ones being abused. You have to ask if the aim of an addiction treatment program should be to maintain a person on an addictive substance. Is there really no better solution?
Some people have also questioned whether or not pharmaceutical companies should be trusted to provide a drug for the treatment of addiction. That’s because many of the same companies that produce buprenorphine also produced opioids that were overprescribed, leading the user into addiction in the first place. Should these companies profit both from creating addiction and from treating it?
Talking to some people in this field, you might get the impression that no other form of opioid addiction treatment will be successful. In fact, many addiction recovery professionals talk about success as consisting of “compliance.”

What is compliance? It means taking your medication as prescribed or following your treatment recommendations. When a person in treatment for opioid addiction takes their buprenorphine/methadone/buprenorphine-naloxone as prescribed, they are considered to be compliant. They are also considered to be a success story. But this is despite the fact that they have not yet recovered from their dependence on an opioid. And the fact that they must consume an addictive substance every day.
How does “compliance” compare with the true freedom found in abstinence-based recovery?
Some of the Problems with Buprenorphine as Long Term Treatment
In America as well as other countries, buprenorphine formulas are readily available on the illicit market. They may be obtained and used for self-treatment of addiction as a substitute when the person’s preferred opioid is unavailable, or to get high, although it is few people’s drug of choice. More than half the people surveyed (who stated that they were addicted to an opioid) reported that they had used buprenorphine diverted from medical use.
Finland’s experience with buprenorphine provides a look at what can go wrong with using this drug as a solution. In the late 1990s, the country’s heroin supply from Afghanistan decreased. Finland’s heroin users turned to buprenorphine as a solution and this prescription drug soon replaced heroin as the most-used drug among people looking for addiction treatment. Eighty percent of users were injecting it and most of these people were also abusing other substances.
Another report in Emergency Medical News noted that in Scandinavian countries, buprenorphine is abused more than cocaine, GHB, or ecstasy, and that it has gained great popularity as a street drug.
Malaysia also struggled with buprenorphine abuse problems. Unfortunately, when this drug was approved for use in addiction treatment, a program was set up so the more people who received the prescription, the more money the prescriber received. This led to a rapid expansion in the number of prescriptions written for this drug by general practitioners (not addiction specialists).
Most of these people in treatment had used heroin before their treatment with buprenorphine began. Then, because of the excessive number of prescriptions being written, it was withdrawn from the market. It was replaced with a buprenorphine-naloxone mix. A subsequent survey of these patients showed that nearly two-thirds of them resumed heroin use after the plain buprenorphine was withdrawn. The authors of this particular study concluded that the buprenorphine-naloxone mix may have reduced but did not eliminate opioid addiction problems.
What Disclosures Should Be Made to a Family Considering Medication-Assisted Treatment?

When a medication-assisted treatment (MAT) program utilizes buprenorphine, here’s some of the disclosures that should be made before a family or individual commits to it.
- Buprenorphine is an opioid. In some circumstances, it is used as a painkiller. It acts on the same parts of the body’s nerve cells like other opioid such as heroin or oxycodone.
- It has the same effects as heroin, specifically, pain reduction, feelings of well-being or pleasure, and respiratory suppression. But these effects are less intense.
- Buprenorphine also has a psychoactive effect, meaning that it artificially modifies the patient’s mental condition.
- The drug also causes some of the same symptoms as morphine abuse, such as constricted pupils, sleepiness, and itchy skin, anxiety, constipation, dizziness, headache, nausea, and sedation.
- According to the National Institute on Drug Abuse, when a buprenorphine formula is prescribed, it is supposed to be prescribed “as part of a comprehensive treatment plan that includes counseling and participation in social support programs.” But as reported by the Christian Science Monitor, “not all prescribers run reputable practices that follow such protocols.” They simply prescribe the drug, sometimes indefinitely.
- It is possible to fatally overdose on buprenorphine or a buprenorphine/naloxone mix.
- Mixing buprenorphine with alcohol, benzodiazepines (Valium, Xanax and others), sedatives, tranquilizers or other opioids can be fatal.
- Buprenorphine can pass into breast milk. And when a pregnant woman has been medicated with buprenorphine, her child may suffer neonatal opioid withdrawal syndrome after birth.
- If a person stops taking this medication, they will experience opioid withdrawal symptoms. These symptoms can include anxiety, depression, night sweats, fatigue, nausea, restlessness, joint and muscle pain, inability to sleep, cramps, vomiting, diarrhea, cravings, lack of sexual interest, lack of motivation. In a few cases, this withdrawal may trigger psychosis.
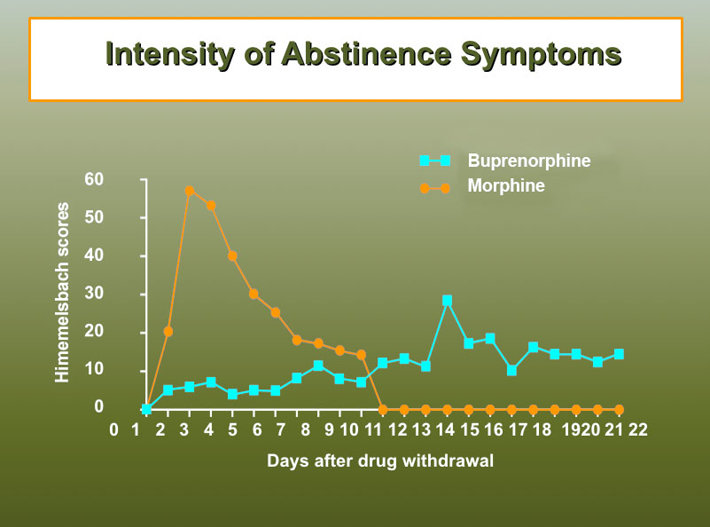
When a person goes through withdrawal from morphine, heroin or oxycodone, withdrawal is likely to last a week or slightly more. But withdrawal from long-term buprenorphine use in addiction treatment can last several weeks to several months. You can see evidence of these longer-lasting symptoms in this chart from the United Nations Office on Drugs and Crime. [Module 1, workshop 1 — PDF]
Another Choice: Short Term Bupinorphine Taper
Some drug rehabs utilize buprenorphine as a short bridge from addiction to illicit opioids like heroin or prescription opioids like hydrocodone. This method of use avoids many of the problems associated with lengthy (or even interminable) use of the drug. It can help a person ease out of their prior lifestyle and into recovery, and ease the effects of withdrawal on a body that may still be struggling with the damaging effects of long-term opioid abuse. While this method has produced positive results it does pose some risks and prolongs the treatment process. For this reason, it’s nearly always better to provide a drug-free supportive approach to withdrawal management.
When choosing addiction treatment, it pays to get educated on the different types of programs available. Admittedly, this can be very difficult because of the urgent need to get an addicted person safely into a rehab. Calling on other family members who might be able to help with this research can assist a mom, dad, sibling, or another caring person in making the right decision on behalf of their loved one.
Sources:
- https://www.drugabuse.gov/publications/effective-treatments-opioid-addiction/effective-treatments-opioid-addiction
- https://www.npr.org/sections/health-shots/2018/09/28/652546095/drugmakers-play-the-patent-game-to-lock-in-prices-block-competitors
- https://www.csmonitor.com/USA/Society/2014/0530/Drugs-for-treating-heroin-users-a-new-abuse-problem-in-the-making
- https://www.sciencedirect.com/science/article/pii/S0376871618307245
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4177012/
- https://journals.lww.com/em-news/Fulltext/2009/01000/Buprenorphine__Toxicity_and_Overdose.6.aspx
- https://www.narconon.org/drug-information/morphine/
- https://www.ncbi.nlm.nih.gov/pubmed/20478668
- https://www.narconon.org/drug-rehab/heroin-rehab/signs-and-symptoms-of-heroin-addiction.html
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2851017/
- https://www.aafp.org/afp/2018/0301/p313.html
- https://www.samhsa.gov/medication-assisted-treatment/treatment/buprenorphine
- https://bmjopen.bmj.com/content/5/5/e007629
- https://www.suboxone.com/pdfs/SuboxoneISI.pdf
- https://journals.lww.com/psychopharmacology/Citation/2017/12000/Possible_Psychosis_Associated_With_Buprenorphine.27.aspx
- https://www.unodc.org/unodc/en/treatment-and-care/volume-c-for-trainers.html
- https://www.narconon.org/drug-rehab/opioid-addiction/
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3150159/